
Ouch! What is pain and how to describe it

It’s personal
Understanding physical pain is difficult since we each perceive pain differently. What feels painful to one person may only feel like mild discomfort to another. Such factors as emotional state and overall physical health have been shown to play a significant role in how people perceive, respond to, and describe their pain.
We also can experience more than one type of pain simultaneously, which further complicates a clear description. Understanding and describing types of pain can help your health care provider diagnose and deliver relief.
What is pain?
 Pain is always subjective. Each individual learns the application of the word through experiences related to “injury” in early life. Stimuli that cause pain are the ones most likely to damage tissue, according to biologists. Thus, most bodily pain represents an experience that associates with actual or potential body-tissue damage.
Pain is always subjective. Each individual learns the application of the word through experiences related to “injury” in early life. Stimuli that cause pain are the ones most likely to damage tissue, according to biologists. Thus, most bodily pain represents an experience that associates with actual or potential body-tissue damage.
Pain is characterized by an unpleasant sensation in a part (or parts) of the body that are damaged. At the same time, pain always represents an emotional experience. As a result, trying to come up with an adequate definition of pain is not without controversy. In 1978, after two years of deliberation, the International Association for the Study of Pain (IASP) defined pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
This definition, which necessarily ties pain to a body-tissue or emotional stimulus, is accepted globally by most health care professionals, and has been adopted by several professional, governmental, and nongovernmental organizations, including the World Health Organization.
However, there is no way to distinguish the pain-experience from tissue damage or from some subjective (emotional) reason. This has led many to argue that “pain is pain,” regardless of the initiating source(s).
Pain sensations derive from communication between nerves, the spinal cord, and the brain. Depending on the underlying cause, there are four basic pain experiences, as listed below.
Acute pain
This represents short-term pain that comes on suddenly and has a specific cause like muscle/tendon/ligament injury, broken bones, surgery, dental work, labor and childbirth, cuts, and burns, to name a few. Acute pain goes away once the cause is treated.
Chronic pain
Best estimates suggests that chronic pain affects more than 50 million U.S. adults, and can last for years, ranging from mild to severe on any given day. Some common examples of chronic pain include frequent headaches, nerve damage, low back pain, arthritis, and fibromyalgia (widespread musculoskeletal pain, fatigue, and sleep disturbances). Since chronic pain has been shown to impact quality of life, people living with chronic pain often develop symptoms of anxiety and/or depression.
Nociceptive pain
This represents the most common pain type. Nociceptive pain is caused by stimulation of nociceptors – pain receptors located throughout the body, especially in skin and internal organs that, when stimulated from a cut or other injury, send electrical signals to the brain causing the perception of pain. Nociceptive pain can be acute or chronic and is further classified as somatic or visceral.
Neuropathic pain
This pain seems to come out of nowhere rather than in response to any specific injury. Neuropathic pain results from nervous system dysfunction resulting from muscle damage or nerve(s) deactivation. Neuropathic pain usually describes as burning, freezing, numbness, tingling, shooting, stabbing, or electric shocks.
While diabetes is a common cause of neuropathic pain, other sources for nerve dysfunction that can prompt neuropathic pain include chronic alcohol consumption, accidents, infections, facial nerve problems (such as Bell’s palsy), spinal nerve inflammation or compression, shingles, carpal tunnel syndrome, HIV, central nervous system disorders (such as multiple sclerosis or Parkinson’s disease), radiation, or chemotherapy drugs.
How to describe pain
When describing pain for diagnostic purpose, it’s important to consider six pain-dimensions.
Pain location
 Sometimes pain signals locate at a specific spot that can be identified by touch, or pain can radiate from one area to another, depending on body or limb position. Sometimes pain can be perceived in a different location than the actual source.
Sometimes pain signals locate at a specific spot that can be identified by touch, or pain can radiate from one area to another, depending on body or limb position. Sometimes pain can be perceived in a different location than the actual source.
Being able to point to the exact location of a visceral pain sensation can indicate possible organs involved and give clues to further diagnosis, testing, and treatment options. The illustration here shows the different visceral organs that might associate to a given pain, and thereby provide further diagnostic clues.
Pain quality
Pain quality refers to the specific type(s) of pain perception. Terms like “aching,” “dull,” or “burning” are common pain descriptors. But these terms often mean different things to different people. Here are commonly acceptable descriptor terms to describe different pain perceptions.
- Aching: persistent, dull, or throbbing
- Sharp: sudden, intense sensation at a specific site
- Dull: persistent aching; not sharp
- Burning: stinging or searing
- Throbbing: rhythmic, pulsating
- Stabbing: sharp, piercing
- Gnawing: persistent, irritating pain that “consumes” the affected area
- Shooting: sudden, radiating sensation that travels along a nerve pathway (think sciatica)
- Tingling: pricking or prickling
- Cramping: tight, spasmodic pain in a specific muscle (or muscle region)
- Heavy: pressure or weight in a specific location
Pain radiation – Where does pain go?
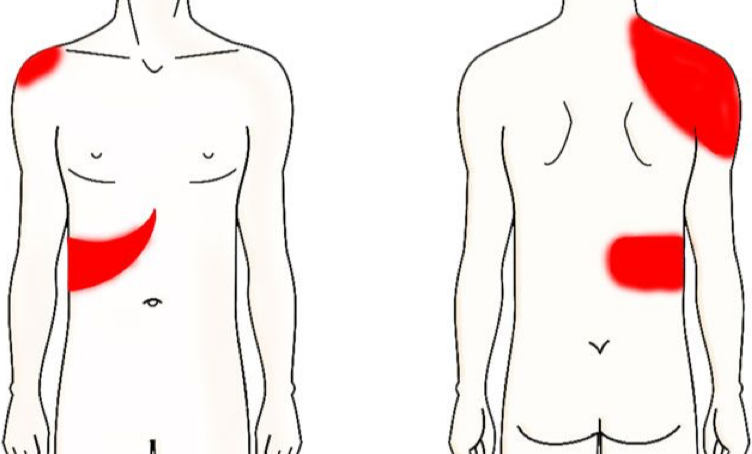 When pain spreads from one body area to another, it is termed “radiating pain.” It often starts in a specific location and then extends to a larger area, and usually feels like a sharp, burning, or tingling sensation. Most often pain radiation results from nerve damage or inflammation, sending pain signals along their pathway. An example of pain radiation is gallbladder pain that sometimes radiates to the shoulder.
When pain spreads from one body area to another, it is termed “radiating pain.” It often starts in a specific location and then extends to a larger area, and usually feels like a sharp, burning, or tingling sensation. Most often pain radiation results from nerve damage or inflammation, sending pain signals along their pathway. An example of pain radiation is gallbladder pain that sometimes radiates to the shoulder.
In contrast, when pain is felt in a different location than the source of the pain, it is termed “referred pain.”
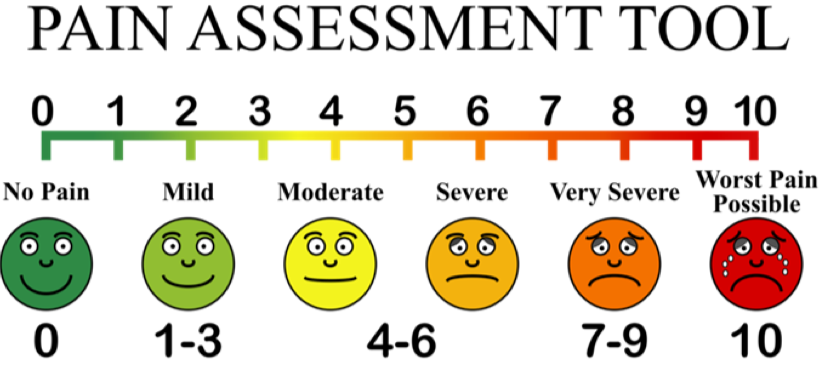
Pain severity – How bad is the pain?
Typically, assigning a number (and descriptor) in the form of a pain scale is used to assess pain intensity. Descriptors include the following terms:
Mild: noticeable but not overly disruptive
Moderate: disrupts normal daily activities
Severe: debilitating enough to prevent normal functioning
Intense: strong, powerful
Agonizing: extremely painful and distressing
Excruciating: unbearable
Pain Timing – When does pain occur?
When pain occurs, how long it lasts, and any daily variations can provide valuable clues about its cause and progression. Pain can be constant, intermittent, or waxing/waning. It also can fluctuate during certain times of the day.
Alleviating factors – What triggers and stops pain?
It is important to be able to describe the onset or triggers for pain as well as being able to describe what you can do to alleviate pain symptoms. This information can help diagnose underlying causes for the different types of pain.
Triggers are specific activities or conditions that can incite or exacerbate the onset of pain. These can include anything from emotional stress, food, or different physical activities. Identifying pain triggers can help manage pain more effectively. More importantly, knowing those triggers may help you avoid pain altogether.
References
- Alcock, M.M. “Defining pain: past, present, and future.” Pain 2017;158:761.
- Anand, K.J. Craig, K.D. “New perspectives on the definition of pain.” Pain 1996;67:3.
- Anand, K.J.S., et al. “Consciousness, behavior, and clinical impact of the definition of pain.” Pain Forum 1999;8:64.
- Brodal, P. “A neurobiologist’s attempt to understand persistent pain.” The Scandinavian Journal of Pain 2017;15:140.
- Cunningham, N. “Primary requirements for an ethical definition of pain.” Pain Forum 1999;8:93.
- Fields, H.L. “Pain: an unpleasant topic.” Pain 1999;Suppl 6:S61–S69.
- Ford, A.C., et al. “Chronic visceral pain: New peripheral mechanistic insights and resulting treatments.” Gastroenterology. 2024;166(6):976.
- Freynhagen, R., et al. “Functioning in chronic pain: A call for a global definition.” Pain 2024;165(10):2235.
- Giordano J., Shook, J.R. “Heeding pain’s prescription.” Pain Physician> 2024;27(5):349.
- Jensen, T.S., Gebhart, G.F. “New pain terminology: A work in progress.” Pain 2008;140:399.
- Kissoon, N.R. “Chronic Widespread Pain.” Continuum (Minneapolis, Minn) 2024 Oct. 1;30(5):1427.
- Nugraha, B., et al. “The IASP classification of chronic pain for ICD-11: Functioning properties of chronic pain.” Pain 2019;160:88.
- Raja, S.N., et al. “The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises.” Pain 2020;1;161(9):1976.
- Robinson, C.L., et al. “Pain scales: What are they and what do they mean.” Current Pain and Headache Reports 2024 Jan;28(1):11.
- Rütgen, M., Lamm, C. “Dissecting shared pain representations to understand their behavioral and clinical relevance.” Neuroscience & Biobehavioral Reviews 2024;163:105769.
- Treede, R.D., et al. “Chronic pain as a symptom or a disease: The IASP classification of chronic pain for the International Classification of Diseases (ICD-11).” Pain 2019;160:19.v
- Williams, A.C., Craig, K.D. “Updating the definition of pain.” Pain 2016;157:2420.
- Woo, C.W., et al. “Quantifying cerebral contributions to pain beyond nociception.” Nature Communications 2017;8:14211.
(Lead image: iStock.)


